55 year male with abdominal pain
12/01/22
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
A 55 year old male presented with altered sensorium and pain abdomen.
K.Lasya Mithra, 9th semester
Roll No: 50
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
CASE:
A 55 year old Male came to hospital with
CHIEF COMPLAINT:
Abdominal pain since 5 days
Shortness of breath- 2 days
Altered sensorium- 1 day
History of present illness:
Patient was apparently asymptomatic 2 weeks back then he developed abdominal pain after taking alcohol continuously for 3 days . It is sudden in onset and gradually progressive and dragging type , non radiating which aggravated on alcohol intake and relieved on medication.He had an episode of vomiting after intake of alcohol for 3 days which is non bilious , non projectile water as content.
On jan 8th,
He developed severe abdominal pain associated with altered sensorium and presented to our hospital.
He also complained of shortness of breath from 2 days which progressed from grade 2 to grade 4.
history of weight loss also from 1 year.
Past history:
A known case of diabetes since 2 years on regular medication .
History of TB diagnosed 3 months back and on regular medication.
Not a known case of hypertension,asthma,epilepsy,CVD.
Personal history:
Appetite - normal
Diet - mixed
Bowel and bladder - regular and there is increased frequency of urine seen when sugar levels are increased .
Not sleeping adequately since 2 days
Alcohol consumption since 30 yrs ,he drinks continuously for 3 days of 1 full bottle and doesn't consume for 10 days.His last binge of alcohol was on jan 6th - 650 ml.
History of tobacco smoking since 25 yrs.( smokes - 3 to 4 beedis per day.)
Family history:
Not significant
General examination:
On presentation , patient is conscious ,not co operative ,not oriented to time place person
Poorlybuilt and poorly nourished .
- GCS : score 10
Eye opening - 4
Verbal response - 3
Motor response - 3
- Pallor : present
- Icterus : absent
- Cyanosis : absent
- Clubbing : absent
- Lymphadenopathy : absent
Vitals:
Pulse - 90bpm
RR - 22 cpm
Bp- 140 / 70 mm hg
Temperature- 97.4°c
Systemic examination:
Abdominal examination-
INSPECTION:
Shape – scaphoid, flat,not distended
Umbilicus – central and inverted
Skin – No scars, no sinuses,no striae, no nodules, no dilated veins.
All quadrants are equally moving with respiration ,
no visible gastric peristalsis.
PALPATION:
No local raise of temperature.
Tenderness not elicited.
Liver-
Not palpable
Spleen-
Not palpable
Kidney-
Bimanually Not palpable
PERCUSSION:
Fluid Thrill/Shifting dullness - not elicited
Liver span - 6cm
AUSCULTATION:
Bowel sounds are heard.
EXAMINATION OF OTHER SYSTEMS
CARDIOVASCULAR SYSTEM:
Apex beat heard at 5th intercoastal space medial to mid clavicular line.
S1, S2 are heard, no added murmurs.
RESPIRATORY SYSTEM:
Trachea- central
Bilateral air entry present
Normal vesicular breath sounds heard.
NERVOUS SYSTEM:
Altered sensorium, irrelevant talking and unable to recognise his wife and he is pulling away the cannula.
Higher mental functions normal.
Cranial nerve examination- normal
Meningeal signs were absent.
Cerebellar functions normal.
Sensory examination: sence of fine touch, vibration, coarse touch are normal.
Motor examination:
Power: upper limbs: 5 bilaterally
Lower limbs: 5 bilaterally.
Tone: Normal
Reflexes: R. L
Biceps:. N. N
Triceps:. N. N
Knee. N. N
Ankle: N. N
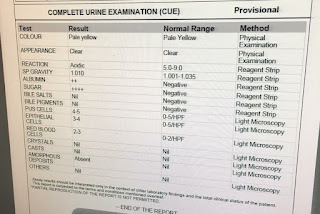
INVESTIGATIONS:
On jan 8th,
GRBS : inj HAI 6IU IV/STAT followed by insulin infusion.
5:30-600 mg/dl
7:30- 390 mg/dl
8:30-380 mg/ dl
9:30- 383 mg/ dl
10:30- 382 mg/dl
11:30- 260 mg/ dl
12:30- 210 mg/dl
1:30- 220mg/dl
2:30- 206 mg/ dl
3:30- 207 mg/dl
4:30- 147 mg/dl
5:30- 77 mg/dl
6:30- 121 mg/dl
7:30- 131 mg/dl
ULTRASOUND (abdomen) REPORT:

On 9 th jan :
Vitals:
Pulse - 110bpm
RR - 22 cpm
Bp- 120 / 90 mm hg
Temperature- afebrile
GRBS - 193 mg/dl
Patient is drowsy and was oriented to time, place and person on repeated questioning.






On 10th Jan :
Pulse - 120bpm
RR - 22 cpm
Bp- 120 / 80 mm hg
Temperature- afebrile
Patient is still drowsy

On jan 11th:
Patient reviewed
Patient is drowsy
Attender denies any irritable behavior and disorientation.
Pain decreased since yesterday
Vitals:
Bp - 110/70 mmHg
PR-102 / min
SpO2 - 98% on room air
Lab investigations-
ABG analysis:
pH -7.44
PCo2 - 25.3
HCO3 - 17.1
Serum urea - 47
Serum creatinine- 0.8
Na+ - 133
K+ - 3.2
Cl- - 94



1. IVF- NS- 1L for 3hrs.
2. Inj HAI 6IU IV/STAT followed by insulin infusion.
3. GRBS monitoring hrly.
4.IVF-5% Dextrose if GRBS<250mg/dl.
5.Inj THIAMINE 100mg in 100 ml NS/IV/BD.
6.Inj OPTINEURON 1 amp in 100ml NS/IV/OD.
On 12 th jan:
Patient is conscious, coherent and well oriented to time, place and person.
Vitals:
Grbs:160mg/dl
Bp:120/80mmhg
PR: 94bpm
Spo2: 99%@room air
RR : 20 cpm
Treatment:
1.IVF- NS,RL- @150ml/hr
2. Inj HAI AND NPH ACCORDING TO GRBS
3.Inj THIAMINE 200mg in 100 ml NS/IV/BD.
4.Inj OPTINEURON 1 amp in 100ml NS/IV/ OVER 30 MIN /OD.
5. INJ PAN 40MG IV/OD
6. INJ ZOFER 4 MG /IV/SOS
7.INJ LORAZEPAM 1 amp IM /SOS.
On jan 13th,
Patient sensorium improved and had mild fever yesterday night.
Vitals:
Grbs:160mg/dl
Bp:120/80mmhg
PR: 94bpm
Spo2: 99%@room air
RR: 20
Treatment:
1.IVF- NS,RL- @150ml/hr
2. Inj HAI SC ACCORDING TO GRBS
3. TAB. ZINCOVIT PO/OD
4. TAB. BENFOMATE PLUS PO/OD
5. TAB. PAN 40 mg PO/OD
6. TAB. ZOFER 4 MG /PO/SOS
7. TAB. LORAZEPAM 2 mg PO/SOS
8. TAB. PCM 650 mg PO/TID
PROVISIONAL DIAGNOSIS:-
Diabetic ketoacidosis with known case of PULMONARY TB(since 3 months)
with altered sensorium secondary to DKA (resolved)


Comments
Post a Comment